
Redesigning how oncologists find clinical trials: from form to conversation
Case Study
Lead Product Designer • Trial Library, 2025–2026 • Launched at ASCO 2026
Overview
Trial Library's Trial Search Platform helps oncologists find relevant clinical trials for their patients and refer them directly to study teams. I inherited the product mid-build in 2023, launched it, then led its redesign as a conversational AI experience ahead of the 2026 ASCO Conference.
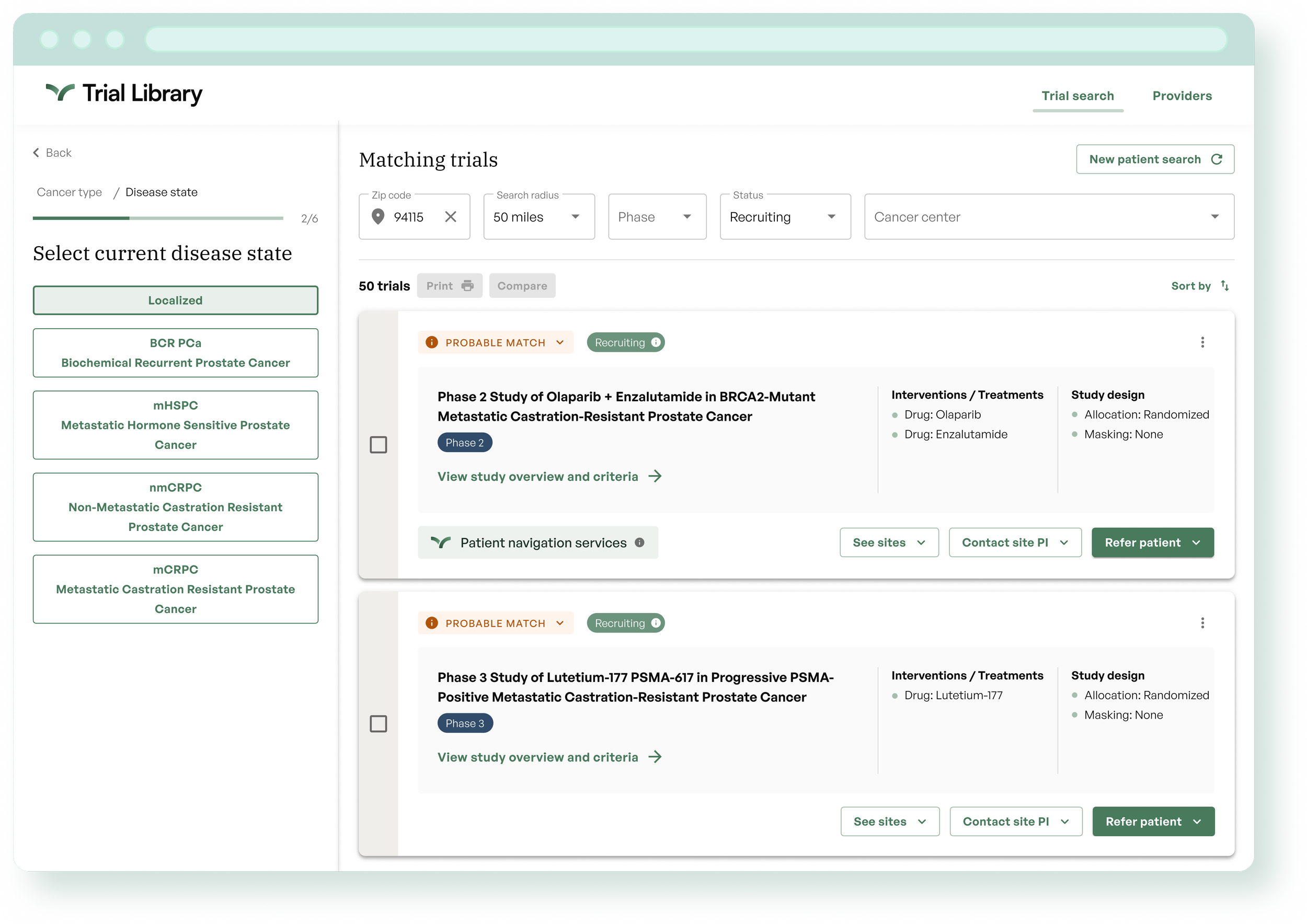
First Trial Search Platform iteration in 2023, questionnaire experience.
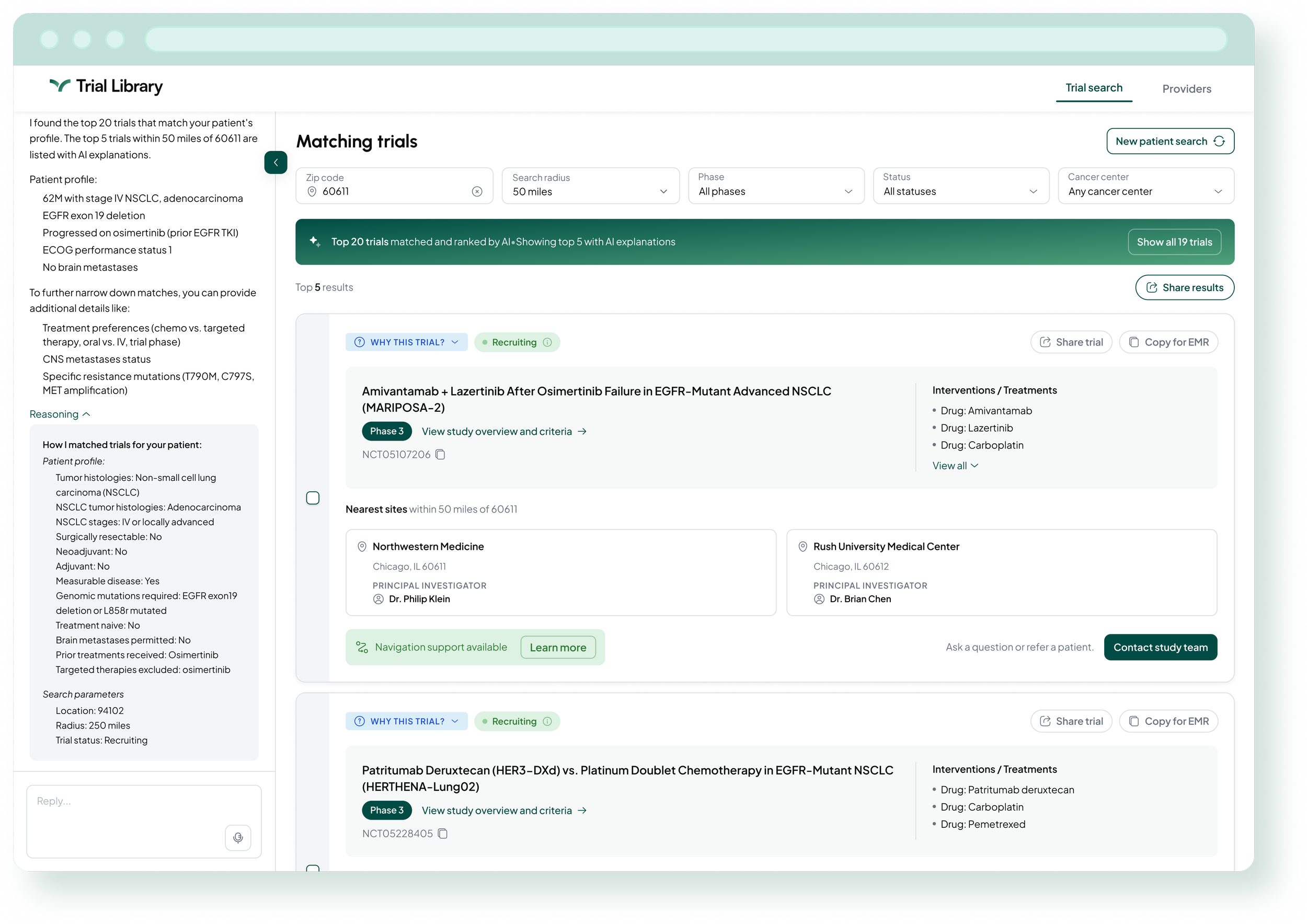
Re-designed conversational AI experience.
The Problem
The original Trial Search Platform launched as an MVP built on design assumptions — we were a new company with no users to test with. The platform guided oncologists through a questionnaire to curate trial results, and it worked. But it was built on hypotheses, not validated workflows. When Series A funding arrived alongside a directive to embed AI more meaningfully in our products, we also gained access to an oncologist advisory group for the first time. The redesign was an opportunity to test those assumptions, learn what was actually missing, and build something grounded in real clinical practice.
Context and Constraints
Two hard constraints shaped every decision. We had to launch at ASCO 2026, a fixed and high-visibility deadline with no flexibility. And the AI directive required interpretation, not just execution. My job wasn't to add AI for its own sake. It was to figure out what AI-first actually meant for a time-pressed oncologist.
My Role
I was the sole designer on this project, partnering closely with our PM who had recently joined the company. Because she was new, I provided the institutional context that shaped our shared decisions throughout — knowledge I had built by inheriting and finishing the original platform. I owned the process end to end: research, interaction model, interface design, and working with engineering from planning through QA.
Research
Before redesigning anything, I ran a usability study with five oncologists and research operations professionals — a pre-session survey followed by a live group feedback session. The numbers told a clear story: navigation and input ease scored 9.0 to 9.2 out of 10, but usefulness scored 7.4. Not one participant would use the product during a patient visit.
Three findings shaped everything that followed. First, results overload was blocking decisions — with 20 or more trials returned, oncologists described needing hours to evaluate options. One participant asked for a ranked shortlist three times in a single session. Second, trust was fragile and specific — generic site names like "Institution 007" immediately stopped referrals, and missing principal investigator information prevented action entirely. Third, the tool was a last resort, not a workflow. Asking colleagues was faster and easier to trust.
The Scoping Decision
I recommended redesigning the search and input experience only, leaving the trial results layer unchanged. The trial cards, with their comparison, print, and referral actions, were working well and represented significant engineering and operational workflow investment. The friction was in how oncologists specified what they were looking for, not in what they did with results once they found them. This focus let us do one thing well rather than two things partially.
Design Decisions
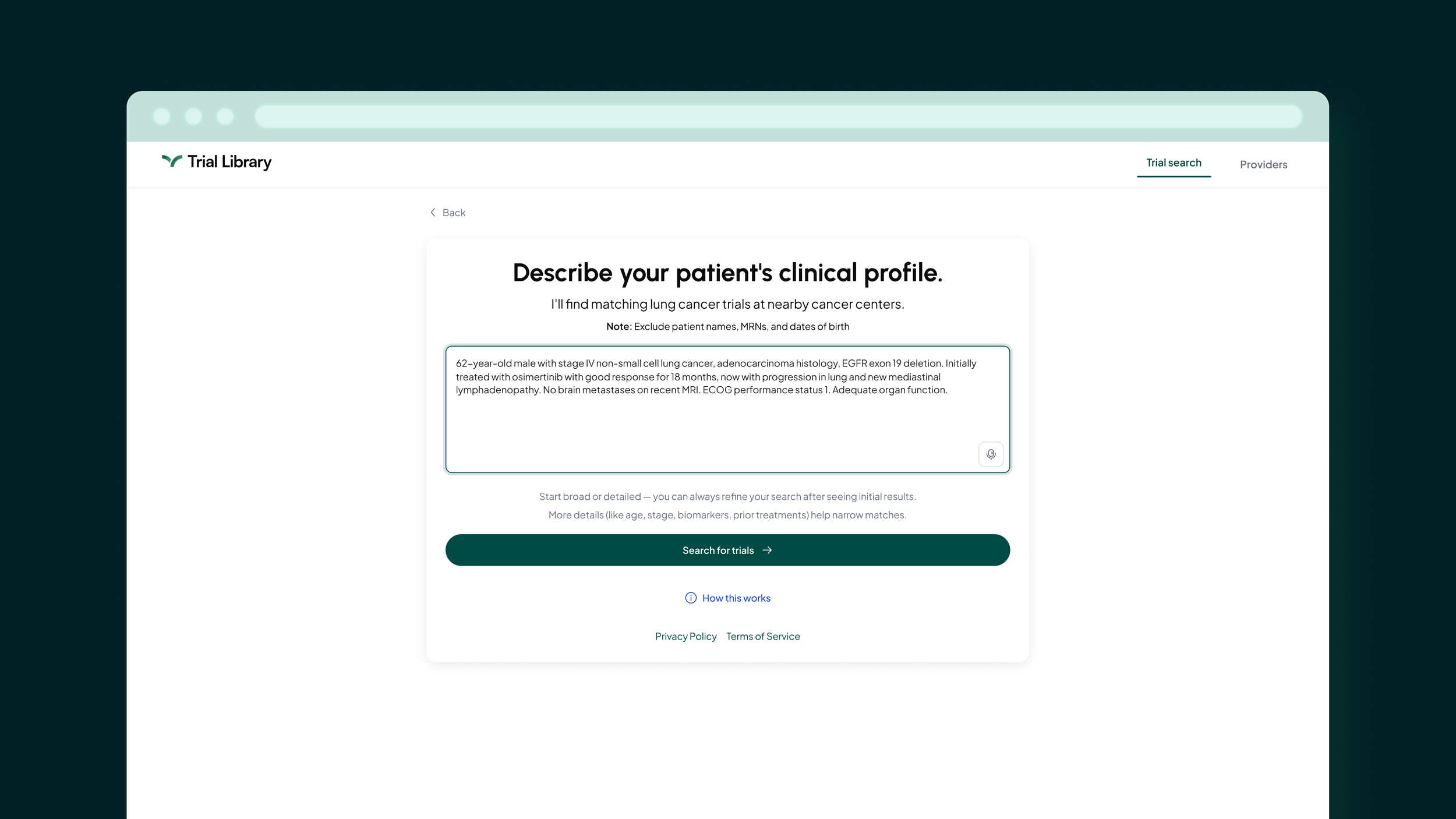
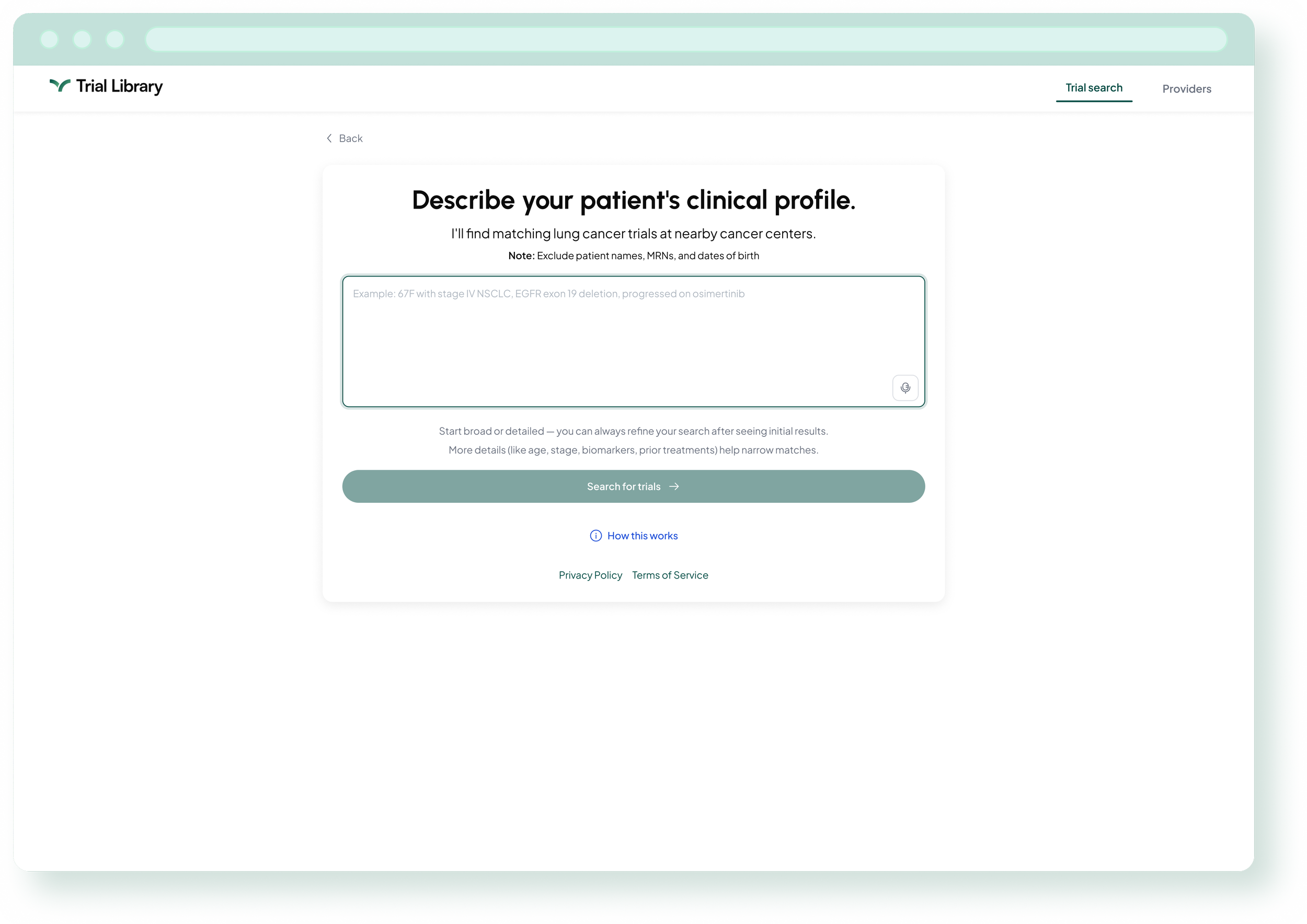
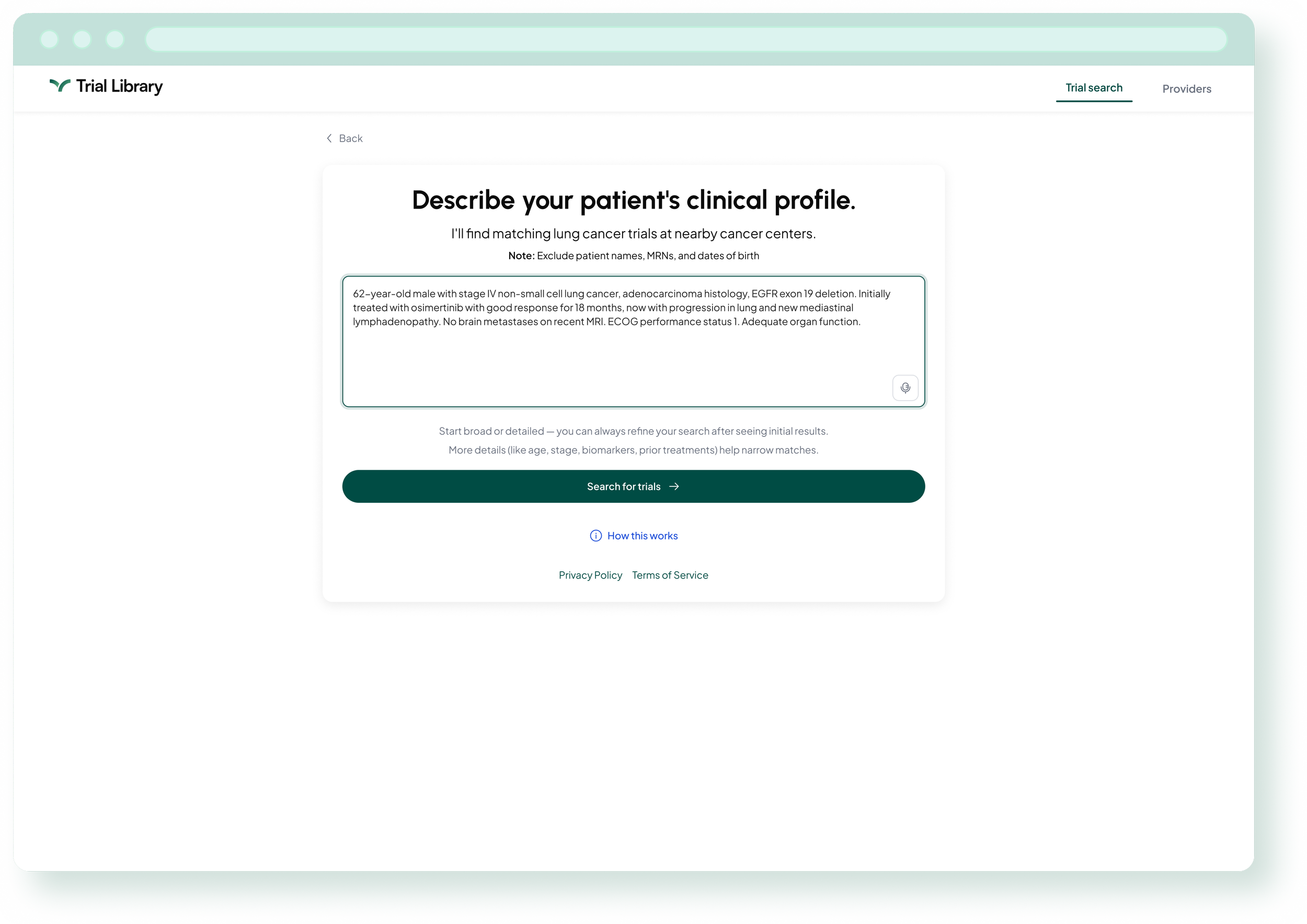
The core question was what "conversational" actually means for a time-pressed clinician. Not open-ended chat, but a single natural language input field that accepts a clinical patient description and returns results immediately, along with follow-up questions to help refine them further. Oncologists could start as broad or as detailed as they wanted. A clinical example in the placeholder text helped guide the interaction, meeting users in the language they already speak.
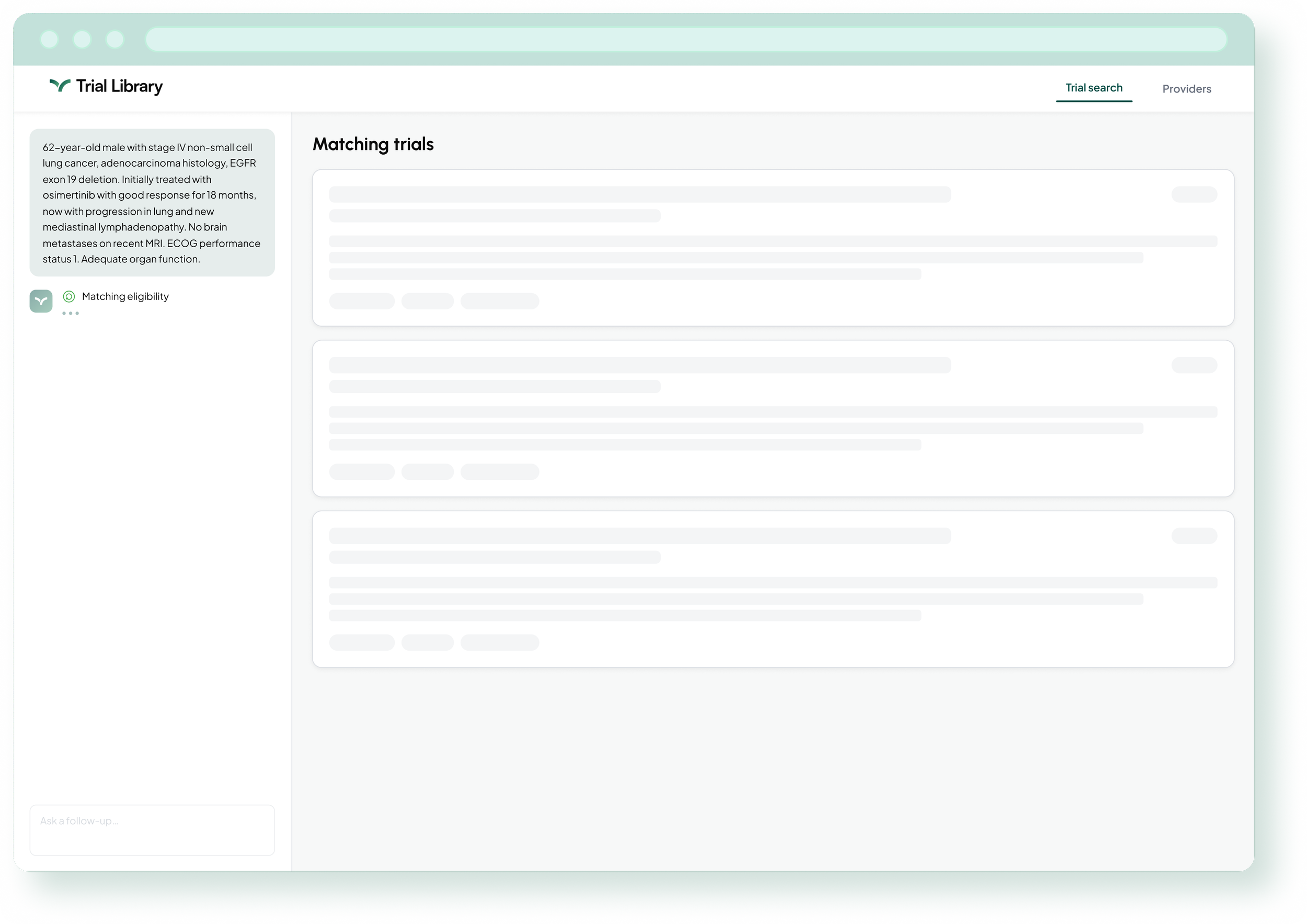
The Thinking State
Between input and results, I designed a progressive thinking state showing the model's processing steps in sequence: matching eligibility, checking location details, ranking results. Research showed zero participants would use the tool during a patient visit, partly because waiting for opaque AI felt uncertain. Making the model's work visible reduced that anxiety and gave oncologists something meaningful to read while results loaded. I provided detailed animation specifications to engineering for how each step should sequence and reveal.
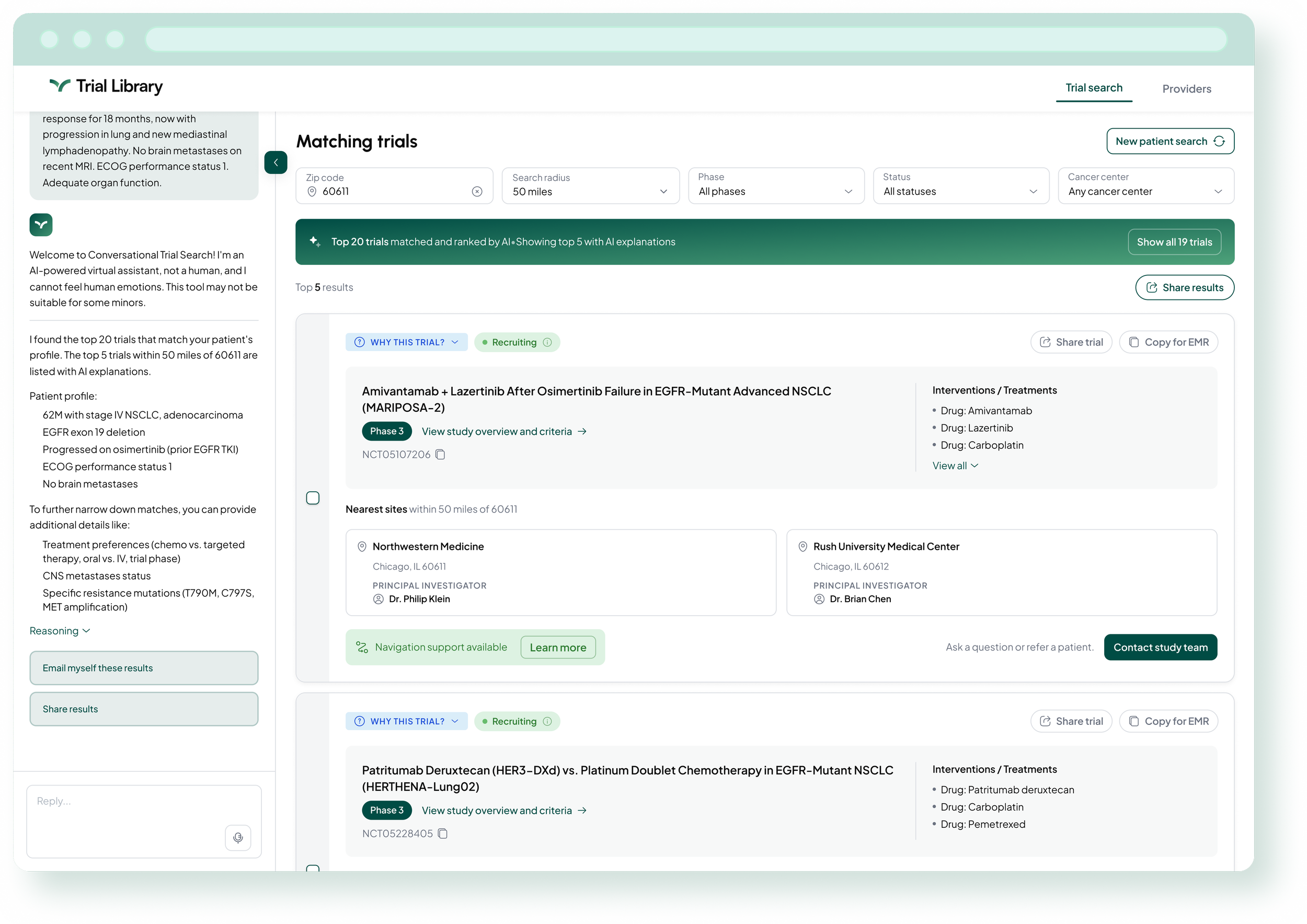
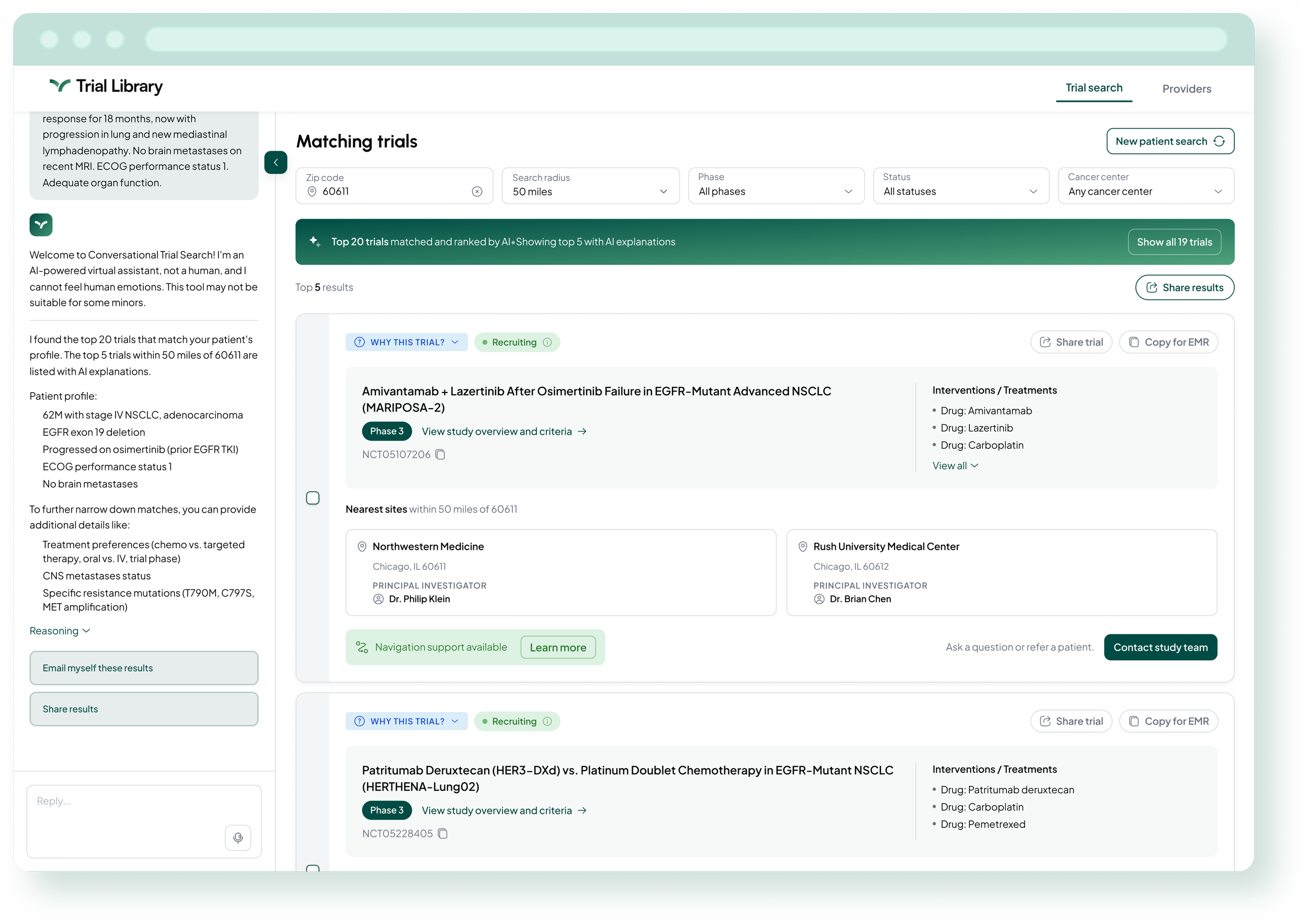
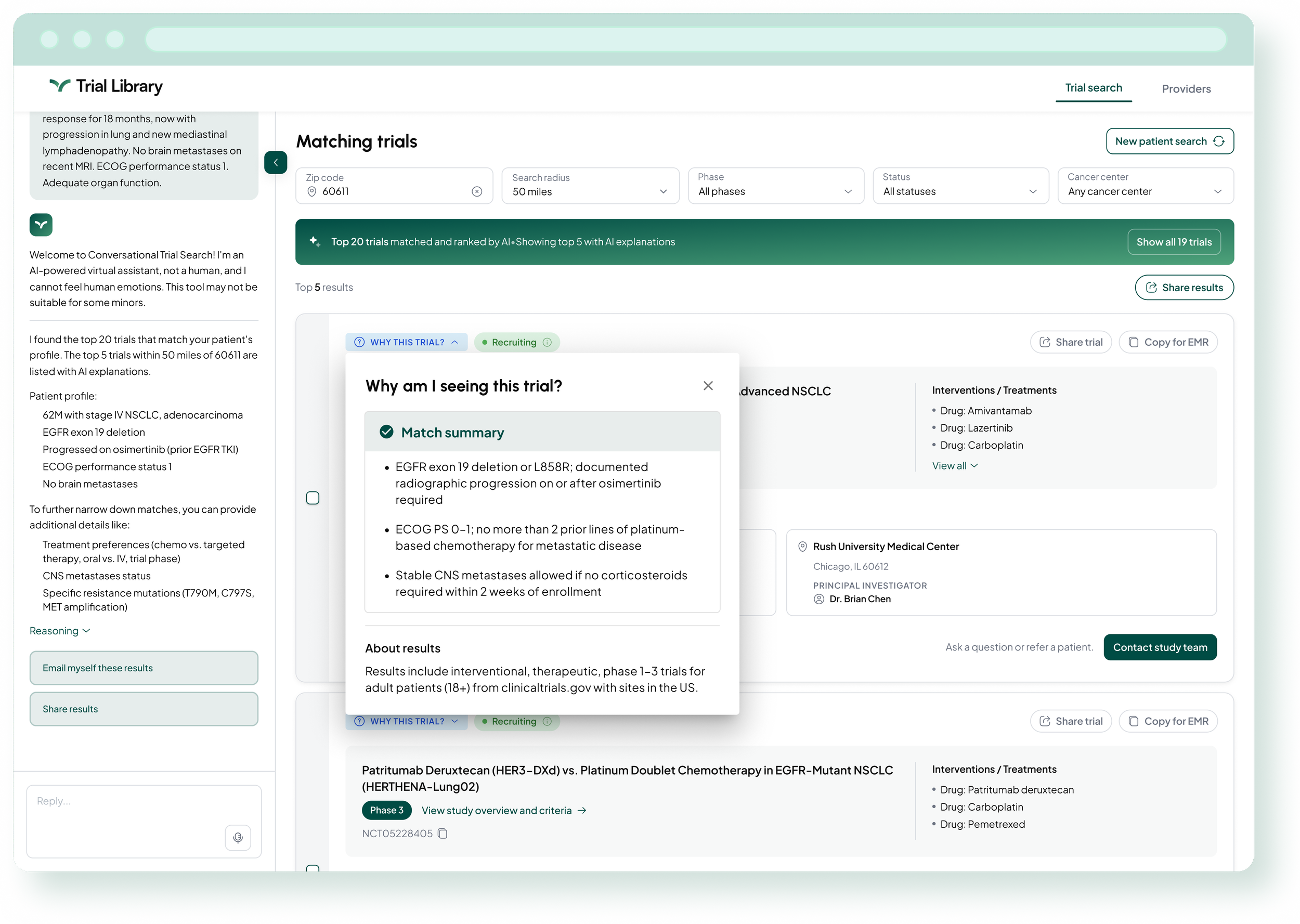
The Response Layer: Building Trust
Research showed oncologists would stop using a tool the moment they caught a single inaccurate result. Trust had to be designed in. I built four components working together as a system: a patient profile summary to verify the model understood the input before results appeared; numbered clinical questions to help narrow to the most relevant trials without starting over; an expandable “Reasoning” panel showing the model's matching logic; and a "Why this trial" button on each result card explaining exactly why that trial was included. Engineering's initial build omitted all four. The PM and I advocated through multiple cycles until they were implemented.
Outcome
Multiple physicians tried the platform and responded positively, describing the experience as fast, user friendly, and intuitive. Their feedback also surfaced ideas for future improvements, including voice input and the ability to share results with colleagues, both of which are on our roadmap.
Reflection
The research revealed something I had not fully anticipated. The questionnaire was not the only problem — the bigger blockers were results overload and the lack of decision support once oncologists had their results. Solving the input experience without addressing those issues would have shipped something that looked different but felt the same.
Getting the response layer built required more advocacy than it should have. The designs and specs were there from the start, but competing engineering priorities meant those details did not make it into the initial build. It was a good reminder that delivering designs is not the same as delivering outcomes. Staying closely involved through implementation, not just handoff, is something I now build into every project from the beginning.